











Oculo-cardiac Reflex and Oculo-respiratory Reflex
1-Oculo-cardiac Reflex
Definition:
Bradycardia
following traction on the extraocular muscles, especially the medial rectus.
The reflex is
particularly active in children. Bradycardia may be severe and may lead to asystole.
Other arrhythmias may occur, e.g. ventricular ectopics or junctional rhythm.
Bradycardia may
also follow pressure on/or around the eye, fixation of facial fractures, retrobulbar
block (pressure associated with local infiltration), ocular trauma, or
manipulation of tissue in orbital apex after enucleation,...etc. The reflex
has been used to stop SVT with an eyeball massage.
Pathway: (Figure 1)
Afferent pathways
are via the trigeminal nerve (ciliary ganglion to the ophthalmic division of
trigeminal nerve to Gasserian ganglion to the main trigeminal sensory nucleus).;
efferents are via the vagus nerve (afferents synapse with the visceral motor
nucleus of the vagus nerve located in the reticular formation and efferents travel
to the heart and decrease output from the sinoatrial node).
Prophylaxis:
Reduced by
anticholinergic drugs administered as premedication or on induction of
anesthesia.
Management:
If it occurs,
surgery should stop, and atropine or glycopyrrolate should be administered.
Retrobulbar block does not reliably prevent it; local infiltration of the muscles has been used instead.
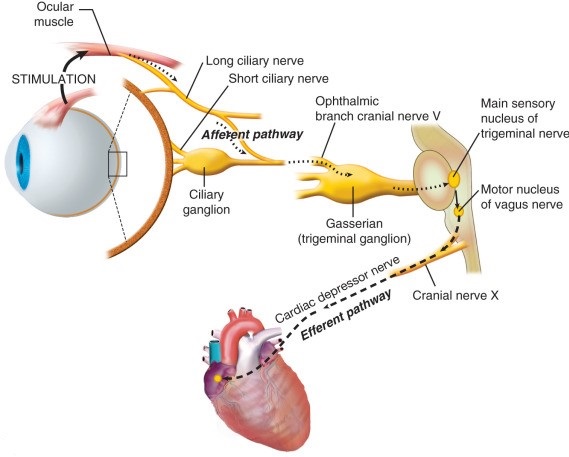 |
| Figure 1: Oculo-cardiac Reflex Pathway |
2-Oculo-respiratory Reflex
Definition:
Hypoventilation
following traction on the external ocular muscles. Reduced respiratory rate,
reduced tidal volume, or irregular ventilation may occur.
Pathway:
Thought to
involve the same afferent pathways as the oculocardiac reflex, but with
efferents via the respiratory centers.
Heart rate may
be unchanged, and the reflex is unaffected by atropine.











